Article Text

Abstract
Objectives Population ageing and increased care needs lead to adults making consequential medical decisions for others, potentially impacting treatment and end of life. We aim to describe the prevalence of medical decision-making by proxy among the national population and associated demographic and care factors.
Methods We designed a cross-sectional online survey with a nationally representative adult cohort with an 80% participation rate. 311 Singapore residents completed the survey.
Results 73% of respondents reported having ever assisted others with medical decisions, while 58% have ever assisted with activities of daily living (ADLs), and 88% with instrumental ADLs (IADLs). Having a digital caregiver account, having a lasting power of attorney as a donee and assisting with ADLs and IADLs are significantly associated with proxy medical decision-making. Gender, ethnicity, income and age did not appear to have a significant impact.
Conclusions A majority of Singapore adults assist others with caregiving tasks and medical decision-making. These helping behaviours are often performed informally, which may increase decisional burden for caregivers and potential abuse of power.
- Advance Directives
- End of life care
- Clinical decisions
- Family management
- Advance Care Planning
- Proxy
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
It is known that caregivers often make decisions on behalf of patients, but the prevalence, type of medical decisions and factors associated with making such decisions are not known. A study on the characteristics of individuals who make medical decisions on behalf of others was needed to understand the prevalence of helping behaviours and factors associated with them.
WHAT THIS STUDY ADDS
This study provides data on caregiving and medical decision-making by Singapore adults on behalf of others, demonstrating higher-than-expected rates. Making medical decisions by proxy is associated with having a digital caregiver account, having a lasting power of attorney (LPA) as a donee, and assisting in caregiving. This study also grants a picture of healthcare and caregiving literacy in the Singapore population and finds informal caregiving and decision-making (without an LPA or digital proxy account) prevalent, highlighting an opportunity to increase uptake of formalised care arrangements.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Given the high prevalence of assisting others with care duties and decisions, and at times informally as well, support via increasing uptake of digital caregiver accounts, advance care directives and formalising medical decision-making may contribute towards reducing the decisional burden on caregivers and respecting patients’ wishes.
Introduction
In addition to direct physical care, individuals may support friends or loved ones through capacity transfer in financial aspects (such as sharing joint accounts),1 medical decision-making (such as advanced care plans (ACPs)), and financial or legal arrangements; such arrangements include digital caregiver accounts which allows one to access health data and make treatment or care placement decisions for another and lasting power of attorney (LPA), which appoints a donee to make decisions on a donor’s behalf if they lose mental capacity.2 These arrangements document patients’ preferences, reduce contention and improve patient care/satisfaction3 and are increasingly needed in ageing Singapore due to higher care needs.4
Most of these capacity transfers are made to informal (ie, unpaid) caregivers5 and are increasingly engaged digitally, as exemplified in the ‘Gift of Certainty’, a government website encouraging ACP and LPA applications.6 As digital health technologies expand, so do caregivers’ roles and responsibilities, including managing home-based care technologies and navigating patients’ increasing marginalisation as society grows more digitised.7
Relationship between caregiving and medical decision-making
Caregivers are more likely to be female, often daughters8 and chosen by care recipients.9 Caregivers are often involved in making important, high-stakes medical decisions (defined as those surrounding care or end of life (EOL)) for patients10; their involvement in decision-making has been linked with illness care involvement.11 There are concerns about caregivers abusing such decision-making power, acting against patients’ wishes or overriding professionals’ authority.12 Research on medical decision-making delegation is often patient-centric, finding that patients often choose companions or children as proxy decision-makers13 and delegation to informal caregivers occurs more often with older, male, less educated and poorer patients.14 Surveys on caregivers’ perspectives of their involvement in care roles and decision-making for other adults are rare.
In Singapore, the most common informal caregivers are adult children of seniors,15 with about half receiving assistance with care tasks from an employed domestic worker/maid.16 However, formal paid caregivers largely do not make decisions for patients, retaining this decisional burden for informal family caregivers.17 Locally, informal caregivers are involved in making medical decisions with and for patients, especially around EOL and life-extending treatment.12 18 However, less is known about how demographic, legal arrangement and care involvement factors are associated with medical decision-making on behalf of others. Hence, it would be worthwhile to study in Singapore the factors associated with high-stakes medical decision-making on behalf of others. As mentioned above, the literature suggests that making medical decisions for others would be influenced by age, gender, income, ethnicity and involvement with physical caregiving.
Research aims
Our team was interested in ascertaining (1) the prevalence of proxy medical decision-making and formalised care arrangements (such as LPA and digital finance or caregiving accounts) among adults in Singapore and (2) the demographic and behavioural factors associated with proxy medical decision-making. Thereafter, we would ascertain the extent of such helping behaviours and whether they are engaged formally or informally. Answering these questions would help explore implications such as caregiving or decision-making burden by caregivers, lack of accountability or even potential abuse of power, which may help guide clinicians and policy-makers in supporting patients and their caregivers.
Methods
Our team undertook a survey of the Singapore adult population focused on involvement with caregiving assistance, proxy medical decision-making and formalised care arrangements, with 107 questions. The findings in this paper focus on adults making medical decisions on behalf of other adults aged 21 years and above. The survey is available in online supplemental material A. The Checklist for Reporting Results of Internet E-Surveys Checklist can be seen in the Research Checklist.
Supplemental material
In this section, we describe the definitions of the terms used, the survey design and sources of the items we used, where available. Where possible, we have rounded percentages to whole numbers for clarity.
Language and definitions
In this survey, we defined a proxy as someone who carries out tasks on behalf of another adult. Tasks were divided into physical and digital tasks. A delegator is an adult who requires help with these tasks; however, a simpler language of ‘helping another adult’ is used to identify the delegator in the survey. Additionally, we used this phrasing because we wanted participants to distinguish helping behaviour from parenting duties where a person below 21 years old is helped.
We define delegation formally through established authorisations such as LPA, ACP and digital caregiver accounts. Practically, proxies or caregivers may assist in medical decision-making through less formalised methods, such as sharing credentials/using the account of a delegator or influencing medical decisions without formal agreements.
Survey design
We included predictors previously identified in the literature, such as gender, ethnicity, education, as well as other potential factors like housing, age, religion, marital status and sibling order. Survey items were not randomised, and adaptive questioning was employed to make the survey less complex for respondents. Completeness checks were built into the survey instrument. Participants could review and change their responses with the review function.
We adapted the activities of daily living (ADLs) and instrumental ADL (IADLs) scales to assess respondents’ assistance with others’ care needs. These measure functional assistance in six basic activities (washing, dressing, feeding, toileting, walking/moving and transferring) that comprise independent living and eight additional functional areas of living (such as housekeeping, cooking and managing laundry, among others), respectively. We added an item on assisting with digital tasks (such as logging onto mobile apps, operating applications, checking emails and changing device settings) under the IADL basket. In adapting these scales for respondents, we first describe the task, then ask the highest frequency ever of help respondents have offered to others, ranging from daily, weekly, monthly, yearly and never.
We next asked about owning a caregiver digital account, which grants respondents decision-making power through an online portal, and whether respondents have LPA arrangements with the person they are helping. We also asked about how they help other adults with financial tasks, taking reference from a survey by Latulipe et al in Canada exploring similar tasks, such as online banking.19
We then asked whether respondents have ever helped another adult with high-stakes medical decisions, such as discussing what would make an adult’s life worth living and being involved with EOL decisions, with responses being ‘yes,’ ‘no, but I should have,’ and ‘no, because I didn’t need to.’ These were coded to indicate a decreasing magnitude of assistance with medical decision-making. Our survey focused on any instance of help as opposed to regular help, to gain a more comprehensive view of the helping landscape among adults; limiting ourselves to those helping regularly may miss out on those who had helped episodically or in times past.
To conceptualise high-stakes medical decision-making, we aggregated 13 items regarding becoming a medical decision-maker for another adult, signing documents on behalf of another adult, conversations about what makes another adult’s life worth living, conversations about what another adult would want near EOL and the respondents’ flexibility in making medical decisions for another adult (see online supplemental material B). This resulted in a continuous variable ranging from 0 to 26. These items were based on a caregiver decision-making scale by Van Scoy et al,20 which helped condense questions assessing consequential outcomes for both care recipients and givers. For instance, signing documents on behalf of a care recipient grants considerable power and agency to the caregiver, potentially affecting life-changing decisions. An example survey question coded for high-stakes medical decision-making is:
Supplemental material
Have you ever talked to another adult about what that adult would want if they were very sick or near the end of life?
To conceptualise low-stakes medical decision-making, we aggregated four items comprising assistance with more routine and less consequential medical tasks, such as making appointments for another adult or helping with medications for another adult (see online supplemental material B). These tasks maintain the status quo of care but have less impact on consequential, life-changing decisions. Similar to the items of ADLs and IADLs, respondents are asked the highest frequency they have assisted in such tasks, including daily, weekly, monthly, yearly and never. A sample question is:
I have helped to make appointments for another adult’s medical care.
Recruitment
Survey respondents were recruited through an online survey company between December 2022 and February 2023. We endeavoured to recruit a sample similar to the resident Singapore population by applying demographic constraints aligned to Singapore’s national census during recruitment. Respondents’ demographics were later compared with census data, demonstrating broad similarity (refer to table 1). Informed consent was taken; participants were informed about study purpose and investigators, that personal information would not be taken, the survey would take approximately 40 min to complete, and their response data would be stored for 10 years before disposal. Respondents were compensated with vouchers for their time. Unique participants were ensured using IP addresses. Exclusion criteria were not being residents of Singapore (verified by comparing respondents’ self-report and IP addresses) and being below 21 years of age.
Summary of demographics of survey respondents
Participation rate was 80%. Of those who accessed the survey link, 97% completed the first page and 59% completed the entire survey (overall completion of 47%). Attention checks were built in to ensure response robustness. Cookies were used on the last page, valid for a week, with duplicate entries avoided by preventing users with the same IP address access to the survey twice. A manual log file was also checked for multiple entries. No minimal timestamp was used—we grouped related items across multiple pages and mixed mandatory and optional items to maintain engagement.
Participants
A total of 311 Singapore residents completed the survey, with their demographics summarised in table 1. Only complete surveys were analysed. The survey population was largely similar to the Singapore population based on available census/ministry data,21 so weighing was not applied. Survey respondents had slightly more males proportionally (53% compared with the national 49%), slightly fewer married individuals (57% compared with 62%) and more singles (36% compared with 29%). Those 70 and above were under-represented in the survey, at 1% of the survey population compared with about 12% of the Singapore population. The income curve followed the national pattern, with the largest proportion of individuals in the US$50 000–US$99 000 yearly income bracket, although a relatively higher proportion of survey respondents were in the US$100 000–US$149 000 yearly income bracket (24%) than the national average (14%). Chinese were slightly over-represented (81% to the national 73%), while Indians were slightly under-represented (5% to the national 9%). Survey respondents were more educated, with proportionally more (59%) having degrees or higher qualifications compared with the nation (36%).
Analysis
Linear regression was performed by using R V.4.3.1 to assess the impact of demographic and care arrangements on proxy medical decision-making. We first examined independence of our various demographic and behavioural factors by inspecting correlation matrices.

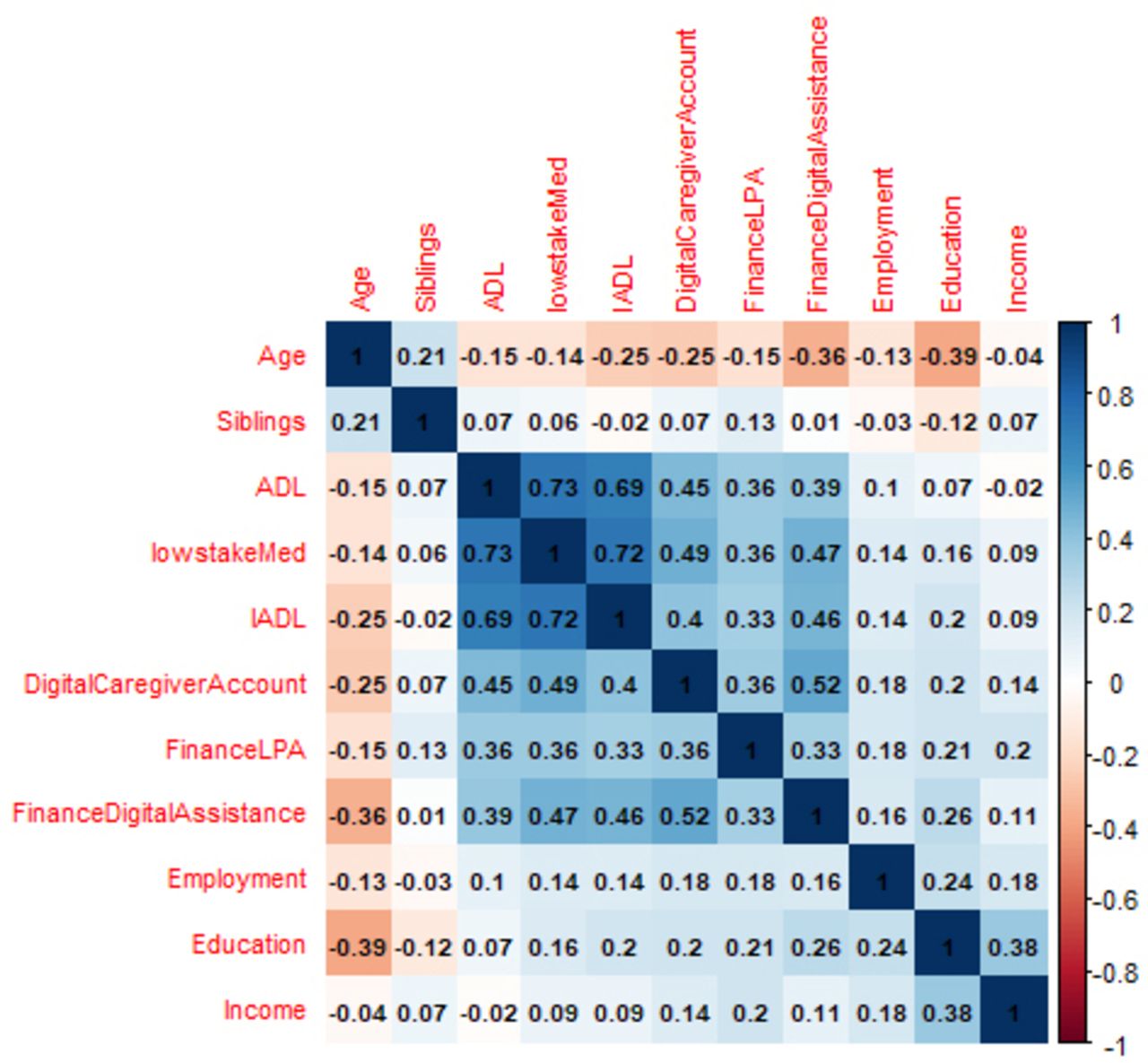
Correlation matrix of predictors for high-stakes medical decision-making on behalf of others, prior to adjustment, demonstrating moderate correlation between assisting with ADLs, assisting with IADLs and making proxy low-stakes medical decisions (0.69–0.73). ADLs, activities of daily living; IADLs, instrumental ADLs.
Figure 1 shows the correlation matrix between variables, which found that assisting with ADLs, assisting with IADLs, and making proxy low-stakes medical decisions were moderately correlated (0.69–0.73). Conceptually, ADLs and IADLs describe distinct sets of tasks. From a caregiver’s perspective, assisting with ADLs involves more direct physical care compared with assisting with IADLs, so we retained both in the regression model. Conversely, as IADLs and low-stakes medical decision-making covered similar tasks, and the latter was less comprehensive with only four items, it was removed from the model due to its correlation with IADLs (0.72).
Only three variables had missing values: gender (<1% missing), ethnicity (3% missing) and siblings (24% missing). The mice package was used to impute missing values using classification and regression trees.22 Thereafter, univariate analysis of association with proxy medical decision-making was run for each variable. We used linear regression for continuous variables, t-test for sex and Krusak-Willis test for categorical variables. Variables with a p value of 0.25 or less were selected for potential inclusion in a multivariate logistic regression model to predict proxy medical decision-making. This p value threshold was suggested to avoid inadvertently excluding important variables.23 We evaluated global fitness of the final model by examining the R-squared and Akaike information criterion (AIC).24
Results
Helping behaviours
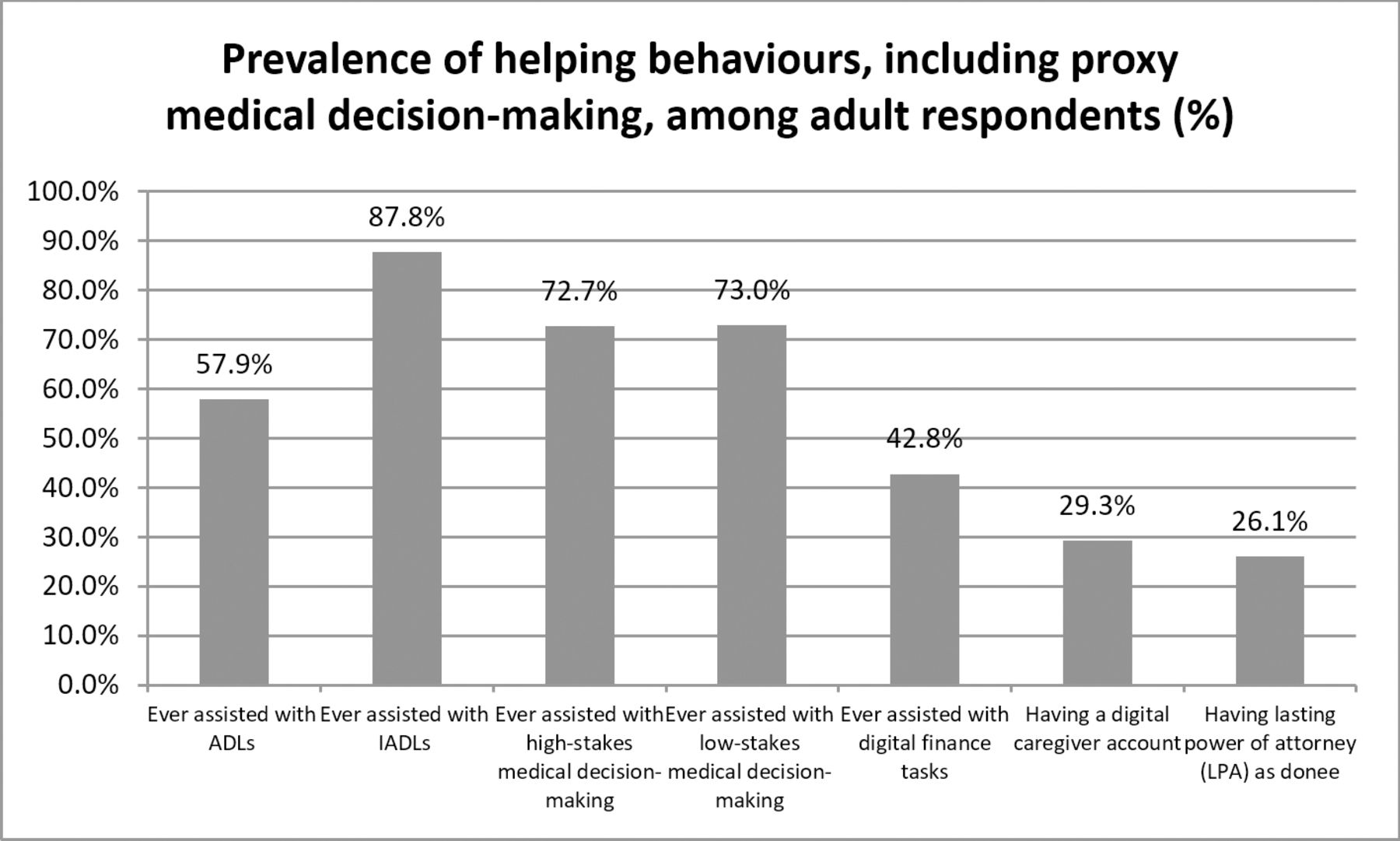
Figure 2 shows the prevalence of respondents having assisted with ADLs/IADLs, digital caregiver accounts, LPAs or high-stakes and low-stakes medical decision-making. More Singapore residents assist others in IADLs (88%) than with ADLs (58%). The rate of respondents having ever assisted with care tasks is higher than expected in the adult population, compared with 8% of respondents of the National Health Survey 2010 reporting they provided regular care or assistance to others (more recent figures are lacking). In addition, 43% of respondents have ever assisted with digital finance tasks, while 26% have an LPA, and 29% have a digital caregiver account.

Univariate association of proxy high-stakes medical decision-making with other factors found age, education, number of siblings, assisting with ADLs, assisting with IADLs, ethnicity, having LPA as donee, assisting with digital finance tasks and having a digital caregiver account to be significantly associated, prior to multivariate analysis. ADLs, activities of daily living; IADLs, instrumental ADLs.
Factors associated with assisting in high-stakes medical decision-making
Regression analysis of factors influencing assisting in high-stakes medical decision-making resulted in the following findings in table 2
Univariate association of proxy high-stakes medical decision-making with other factors
Backwards stepwise removal of variables was applied to the model using AIC. Having a digital caregiver account, having LPA as someone’s donee and assisting in ADLs and IADLs emerged as factors significantly associated with proxy medical decision-making (table 3) in the multivariate model. Gender, ethnicity, religion, marital status and sibling order did not appear to have a significant impact.
AIC regression analysis of factors impacting high-stakes medical decision-making
Discussion
Principal findings
Roughly 73% of respondents assist others with high-stakes and low-stakes medical decisions, which is comparable with literature on caregivers’ involvement with decision-making for patients.25 58% of respondents assisted with ADLs, and 88% with IADLs, higher than the National Health Survey 2010 which found 8% of Singapore adults aged 18–69 provided regular care to friends or family.26 This could be explained by our survey asking if respondents had ever assisted rather than regular and current assistance.
More respondents assist others in IADLs than with ADLs. Adults with established care arrangements, such as digital caregiver accounts or LPA donees, are also involved with making high-stakes medical decisions on behalf of others. Hence, respondents are more likely to assist in less direct/physical forms of care, such as help with finances and medical decision-making, as opposed to physical care tasks. This could be due to formalised or employed caregiving, such as domestic helpers or maids, tasked to meet the physical care needs of patients.15

{kind=link}
{kind=link}
{kind=link}
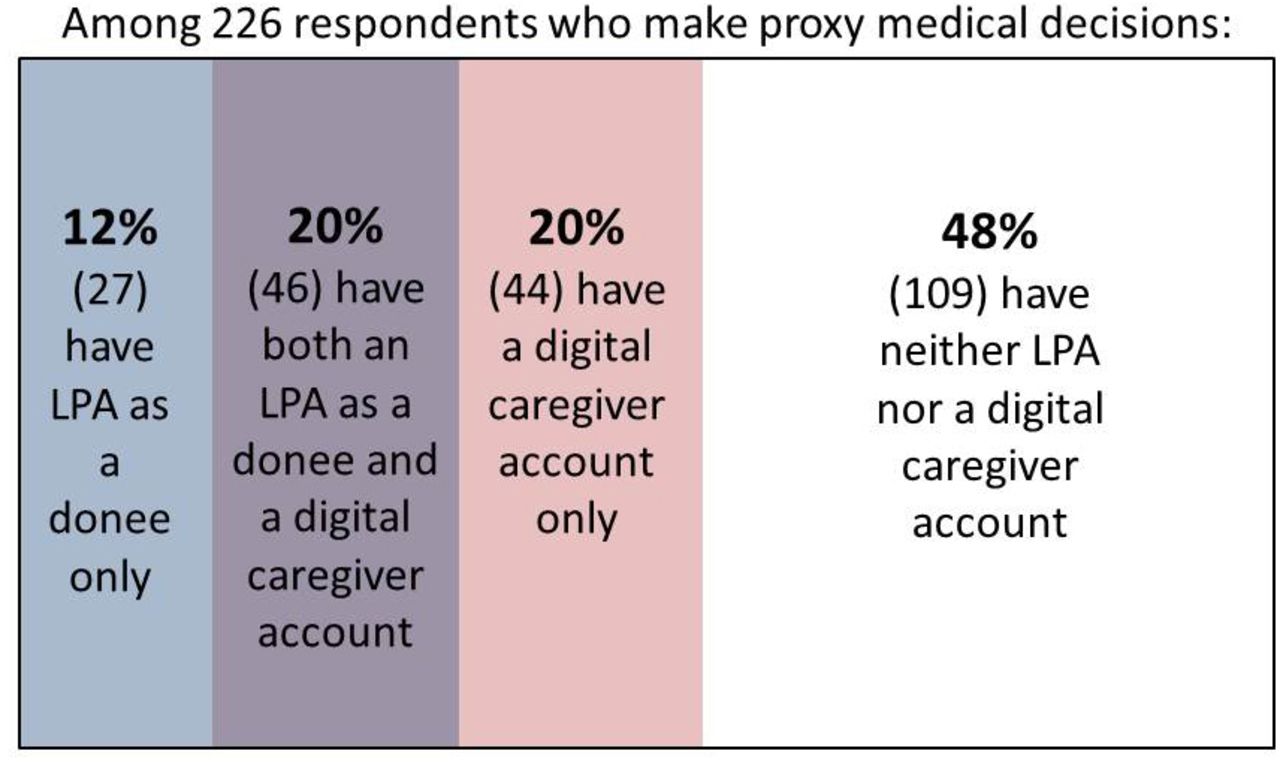
The Venn diagram shows that among those making proxy medical decisions, 48% do not have an LPA nor a digital caregiver account, demonstrating a gap between formalised care arrangements and actual proxy decision-making. LPA, lasting power of attorney.
Our data revealed a significant gap between formalised and actual proxy medical decision-making. Out of the 226 respondents who make proxy medical decisions for others, only 90 (40%) actually had a digital caregiver account and 73 (32%) are actual LPA donees. Close to half of those making proxy medical decisions (48%) do not have any form of formalised care arrangement such as an LPA or digital caregiver account (see figure 3), revealing much of these medical decisions are made informally or without oversight. Ideally, caregiving accounts and formalised delegation through LPA should go hand-in-hand. This disparity highlights the need for increased uptake of formalised arrangements and initiatives to improve education and reduce barriers to such arrangements.
In line with existing literature,11 27 making medical decisions by proxy is associated with involvement with caregiving. However, unlike previous studies,14 27 gender, education, ethnicity and age were not significantly associated. This could hint at a more egalitarian societal with less rigid social norms in determining proxy medical decision-making.
Implications for clinicians and policy-makers
A majority of respondents assist others with medical decisions, which likely increases decision-making burden28 and anxiety/stress on informal caregivers. As Singapore also faces a rapidly ageing society and concurrent increase in caregiving burden, the proportion of those involved in such roles is only likely to increase. This may also increase patient abuse; locally, caregiver stress is a factor commonly implicated in cases of elder abuse.29
In Singapore, support for caregivers is often fragmented, dependent on individuals’ knowledge and uncoordinated.30 We suggest increasing education around the implications of proxy medical decision-making and offering digital caregiving accounts as a way to enhance care delivery while upholding patients’ wishes; this can be done online with caregivers granted tailored access rights,31 through a one-stop portal such as HealthHub, verified by Singpass, a national government digital identity portal.32 Further, crafting advance care directives reduces caregiver decisional burden by establishing patients’ wishes prior to illness or incapacity33—there are opportunities to increase education about and uptake of advance directives, especially in primary care.34
Another finding from our survey is that respondents help others informally—for example, while a majority assist others with medical decisions, 48% do not have any sort of formalised care arrangement such as an LPA or digital caregiver account. This may lead to abuse of power and loss of autonomy,35 such as financial abuse or acting against patients’ wishes.4 With the growing use of technologies like cloud computing and digital account sharing, patients’ data (including medical records) may face threats to data security and privacy against their wishes.36 Low uptake of formalised care arrangements may be due to a lack of awareness or difficulty navigating such platforms—both targeted and national education campaigns can prime caregivers and patients to discuss and document important medical, legal and financial decisions before loss of capacity.
Age, gender, income and ethnicity are not significant determinants of who makes high-stakes medical decisions on behalf of others in Singapore. Instead, those who make such decisions are those who assist with physical and decisional caregiving tasks. This observation may be helpful for clinicians and policy-makers who want to increase uptake of formalised care arrangements like ACPs by targeting education to households with aged dependents. Policy-makers in Singapore have been pushing for increased uptake of such arrangements through campaigns like the ‘Live Well. Leave Well.’ campaign advocating EOL conversations37 and systematic training in hospitals engaging patients or caregivers in ACPs.38 However, ACPs are usually only broached in hospital settings when patients are ill or perhaps already have impaired capacity.39 Hence, it would be helpful to bring advance care discussions into the community, primary care34 and online.40 For example, bringing ACP discussions to current Healthier SG visits, community sites like senior activity centres or active ageing centres, or other important national administrative procedures (such as renewing travel or identification documents), can increase touchpoints for ACP uptake.
Limitations
Owing to the use of an online survey instrument that was conducted in English, there is possibly a bias towards English-speaking, educated and younger survey respondents, which may reduce the representativeness of findings. However, this is mitigated by the effort to assemble a cohort resembling the national population through recruitment constraints. Our goal was to assess the prevalence of helping behaviours and proxy medical decision-making in the general population, not just among identified caregivers, to offer insights into informal caregiving.
Second, this study was based on self-reported helping behaviours, which may suffer from recall or social desirability bias. Some participants may over-report their helping behaviours, which may explain our high prevalence of assisting with care activities or decision-making. However, the prevalence of more formal care arrangements like ACPs or LPAs is comparable with regional and local studies, demonstrating concurrence; hence, the high prevalence of care and decision-making helping behaviours may truly be explained by our question framing as ‘ever-helped’ rather than ‘regularly helping’ in other surveys.
Conclusion
Our research shows a high prevalence of assisting with high-stakes medical decision-making on behalf of others and residents helping more with IADL and decisional caregiving as opposed to physical caregiving. Making high-stakes medical decisions for others is associated with involvement with ADLs and IADLs (potentially adding to caregiver stress), and also with having a digital caregiver account, and having an LPA as a donee. Age, gender, ethnicity and other demographic factors were not significantly associated. Increasing education around the implications of proxy medical decision-making and formalised care arrangements may help increase their uptake, thereby reducing caregiver decisional burden and risk of patient abuse while respecting patient preferences.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and ethical approval was sought and obtained from the National University of Singapore’s Institutional Review Board (Ref: NUS-IRB-2022-412). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to thank Dr Celine Latulipe for kindly sharing the survey instrument from her paper which helped in the development of our survey.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
X @NoreenChanSg, @MervynLimJR
Contributors CZ, PVSP and PSF devised the project and conceptual ideas and designed and implemented the survey. AIHP, CZ, PVSP and PSF jointly crafted the research questions. AIHP ran the analyses and drafted the manuscript and figures. CZ, PVSP, PSF, GCHK and TML reviewed the analyses and helped improve the model. AIHP, CZ, PVSP, NC, MJRL, TML, GCHK and PSF discussed the results and improved on the final manuscript. PSF is the guarantor of this research. All authors have agreed on the final version and meet at least one of the following criteria (recommended by the ICMJE: http://www.icmje.org/ethical_1author.html).
Funding This work was supported by the Singapore Ministry of Heath’s National Medical Research Council Grants (grant numbers NMRC/CG1/009/2022-NUH and CareEco21-0030).
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.