Article Text

Abstract
Objectives To characterise patient-reported financial burden of living with advanced colorectal cancer in Alberta, Canada, as part of a larger prospective cohort study characterising the experiences of people living with advanced colorectal cancer.
Methods Patients were recruited from Alberta’s tertiary cancer centres between January 2018 and July 2020. Enrolled participants were invited to complete the Patient Self-Administered Financial Effects (P-SAFE) questionnaire at 1 month post-enrolment and every 6 months thereafter, until death or end of study (December 2020). The questionnaire captured consumption expenditure, out-of-pocket costs, including travel and parking costs, dissaving strategies and productivity impacts of patients and caregivers over the past 28 days.
Results Of 87 eligible patients, 56 completed at least one P-SAFE survey. They reported an average of $C401 in out-of-pocket costs (eg, medications, vitamins/supplements, devices) over the past 28 days (median $C84, range $C0–$C4475), plus an average of $C249 per 28 days for travel and parking (median $C80, range $C0–$C2680). Patients reported an average of two trips per month to their cancer centre, travelling anywhere from 6 to 500 km one way. 88% of employed patients and 88% of employed caregivers reported impacts on employment; 34% of patients made significant asset decisions (eg, withdrew savings, downsized home). 30% of patients reported high perceived financial burden (ie, ‘somewhat’, ‘large’ or ‘worst possible’ financial difficulty) in the past month.
Conclusions This cross-sectional descriptive analysis suggests that the financial burden of advanced colorectal cancer is high, as evidenced by high out-of-pocket costs, impacts on employment and self-reported financial difficulty.
- Cancer
- Gastrointestinal (lower)
- Outpatients
- Palliative Care
- Supportive care
Data availability statement
Data are available on reasonable request. Aggregate, deidentified data may be made available on reasonable request from the corresponding author. The data are not publicly available, consistent with the ethics approval.
WHAT IS ALREADY KNOWN ON THIS TOPIC
Despite Canada having a publicly funded healthcare system, Canadians living with cancer still experience significant financial challenges. A recent Canadian study showed significant financial burden among a large sample of people living with a variety of tumour types, stages of disease and places of residence.
Less is known about the financial burden experienced by people living with advanced cancer, and if/how financial burden might change as people approach the end of life.
WHAT THIS STUDY ADDS
The financial burden of advanced colorectal cancer is high. Patients reported an average of $C401 per month in out-of-pocket costs; the vast majority of employed patients and caregivers reported impacts on their employment; and one-third of patients made significant asset decisions in response to their financial burden.
This study is also notable for capturing longitudinal financial effects data from patients living with advanced colorectal cancer. While patients report high out-of-pocket costs at baseline, these costs appear to diminish over time, with lower values 6 and 12 months later.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
A multipronged approach involving frontline providers, cancer centres and governments should be considered to mitigate the financial burden of people living with advanced cancer.
Introduction
Despite Canada having a publicly funded healthcare system, Canadians living with cancer still experience significant financial challenges.1 This is because not all aspects of care are fully funded (eg, prescription drugs, over-the-counter drugs), some services have monthly or annual limits, patients (and quite often their family/informal caregivers) are unable to maintain their full employment, and some Canadians often travel significant distances to receive care.2 A Canadian analysis using a cancer microsimulation model and published literature estimated that costs borne by patients with cancer and their families (ie, out-of-pocket costs, time costs related to travel and receiving care, and indirect costs such as lost earnings from employment) amounted to almost $C4.8 billion in 2021.1
A Canadian study by Longo et al surveyed 901 patients with cancer from twenty cancer centres nationally about costs (direct and indirect) related to their cancer treatment.3 Survey participants reported spending an average of $C518 per month on out-of-pocket costs related to their cancer, with some participants spending 50% of their monthly income on these out-of-pocket costs. 29% of patients and 26% of caregivers reported missing time from work (18.0 and 11.5 days off per month, respectively).3 Systematic reviews of the direct and indirect costs of cancer care identified significant burdens borne by patients, caregivers, employers and society.4 5 The impact of this financial strain is significant, with 38%–71% of patients reporting heightened distress from their financial burden.6
The national survey by Longo et al showed significant financial burden among a large sample of Canadians with a variety of tumour types, stages of disease and places of residence. Less is known about the financial burden experienced by people living with advanced cancer, and if/how financial burden might change as people approach the end of life.7 8 This study aimed to characterise patient-reported financial burden of living with advanced colorectal cancer in Alberta, Canada, as part of a larger prospective cohort study, ‘Living with Colorectal Cancer: Patient and Caregiver Experience’, characterising the experiences of this population.9
Methods
Context
The ‘Living With Colorectal Cancer: Patient and Caregiver Experience’ prospective cohort study was conducted from 2018 to 2020 to gather outcome and experience data from patients living with advanced colorectal cancer and their caregivers in Alberta, Canada.9 This study was conducted as part of a larger programme of research (the Palliative Care Early and Systematic Project, www.pacesproject.ca) focused on developing, implementing and evaluating an early palliative care pathway for patients living with advanced cancer. This study was conducted in Alberta’s two tertiary cancer centres (in Edmonton and Calgary), serving patients in urban and rural areas across northern and southern Alberta, respectively (total population 4.3 million in 2018).10
Participants
Patients with advanced colorectal cancer, defined as primary or metastatic colorectal cancer that is unlikely to be cured, controlled or put into remission with treatment, were recruited from outpatient medical oncology clinics focused on gastrointestinal cancers in Calgary and Edmonton from January 2018 to June 2020. Patients were invited to participate by their cancer care provider if they were >18 years of age and met at least one of the following inclusion criteria: failed first line of chemotherapy (disease progression on imaging), unable to receive first line chemotherapy, prognosis of less than 1 year survival estimated by a healthcare provider or patient-reported high symptom burden (any score ≥7/10 on the Edmonton Symptom Assessment System Revised). Language spoken was not an exclusion criterion, with translation available for all study materials.
Data collection
The Patient Self-Administered Financial Effects questionnaire (P-SAFE V.7.2.6) was used to capture direct and indirect costs associated with advanced cancer treatment (online supplemental appendix A).3 An adapted version of the P-SAFE was created for this study that included details on patient demographics (income, employment status, living arrangements), general health, treatments received (chemotherapy, radiation, surgery), level of insurance coverage, employment details, out-of-pocket costs, perceived financial burden, decisions to forego care and time lost from work for patients and their caregivers.3 Some demographics were omitted from the P-SAFE tool as they were collected via other study assessments.
Supplemental material
As per Longo et al,3 out-of-pocket costs were classified by ‘type of expense’ into the following categories: prescription drugs, in-home healthcare (eg, nursing, home health aides), homemaking services (eg, cleaning or cooking), complementary and complementary medicine (eg, acupuncture, homeopathy, naturopathy), vitamins and supplements, family care (eg, babysitting, elder or respite care), other health professionals (eg, physiotherapists, counsellors), accommodations/meals, devices/equipment and ‘other’ costs (ie, all other out-of-pocket costs not captured elsewhere) over the past 28 days. The tool also included questions on work impacts (eg, reduced hours and days out of work) in the previous 28 days, and whether government or employer partial or full salary was available for patients and up to three caregivers.
Study participants were invited to complete the P-SAFE at 1 month post-enrolment, and then every 6 months thereafter until death or study end. The P-SAFE survey was not added to the study until April 2019, so longitudinal P-SAFE data are not available from all study participants. Patients enrolled in the study prior to April 2019 were invited to complete the P-SAFE at the next closest scheduled time point (eg, month 1, month 7, month 13 of their participation) (online supplemental appendix B). The first P-SAFE survey completed by each study participant was considered their ‘baseline’ P-SAFE assessment. P-SAFE surveys were completed with a research assistant either by phone or in person, depending on participant preference.
Supplemental material
Calculations and scoring
As per Longo et al,3 out-of-pocket costs were calculated as the sum of prescription drugs, vitamins/supplements, devices, in-home and other health professionals, complementary and complementary medicine, family care, homemaking, accommodations and ‘other’ costs. Only costs that were self-paid by participants (ie, not covered by insurance or other source) were included. For car travel, imputed travel costs were calculated based on travel distance to the clinic, multiplied by the number of trips and then multiplied by $C0.58/km (Canada Revenue Agency mileage rate at midpoint of recruitment).11 Parking fares (car travel only) were calculated based on the average parking cost per day multiplied by the number of trips in the previous 28 days. The monthly out-of-pocket costs by category represent the mean of all out-of-pocket costs reported in each category.
Categorical impacts on employment were calculated only among those participants deemed ‘eligible to work’, that is, we excluded patients and caregivers who reported being retired or unemployed by choice (eg, self-described as ‘homemaker’) at the time of data collection. Participants were deemed to have a categorical impact on employment if they reported reducing their number of work hours, or being unable to work at all, over the past 28 days. We did not calculate a dollar value for patients’ and caregivers’ lost earnings from employment due to the infrequency with which the question on time lost from work was answered (ie, of the 110 P-SAFE surveys completed, only 13 surveys (12%) reported any hours or days lost from work).
For patient-perceived financial burden, low-burden responses (‘none’ and ‘small’) were compared with higher burden responses (‘somewhat’, ‘large’ and ‘worst possible’), as per the methodology of Longo et al.3
Statistical and data analyses
Information on participant demographics (age, gender, income categories and education), treatment patterns, and the level of burden for participants, including distributions and income effects, is presented as means, medians, SDs and ranges for continuous variables and frequencies and percentages for categorical variables. Patient demographics at baseline were compared by t-test (for age), or by χ2 or Fisher’s exact tests for all other demographic factors. The influence of demographic factors on patient-perceived financial burden was analysed by t-test (for age), or by χ2 or Fisher’s exact tests for all other demographic factors.
Results
Participants
A total of 131 patients were enrolled in the study from January 2018 to June 2020 (42 from Calgary and 89 from Edmonton), with follow-up continuing until December 2020. 44 patients were off-study (deceased or withdrew) prior to roll-out of the P-SAFE survey, leaving 87 patients eligible for P-SAFE completion. 56 patients (64% of eligible), 13 from Calgary and 43 from Edmonton, completed at least one P-SAFE survey during the study (P-SAFE cohort); the median number of surveys completed per patient was 2 (range 1–4) (table 1). A total of 110 P-SAFE surveys were collected between April 2019 and August 2020. 31 patients (36% of eligible) declined to complete any P-SAFE surveys (non-P-SAFE cohort) (online supplemental appendix B).
Patient demographics
Baseline demographics are shown in table 1. No significant differences were observed between participants in Calgary and Edmonton (data not shown).
There were no significant differences in patient demographics between the P-SAFE and non-P-SAFE cohorts (table 1).
P-SAFE completion
Participants chose not to answer some questions, leaving some data fields incomplete (eg, 14/56 participants (25%) did not disclose their family income). The questionnaire took 30–60 min to complete with the research assistant.
Monthly expenditures
56 patients completed at least one P-SAFE survey. We refer to patients’ first P-SAFE survey as their ‘baseline’ P-SAFE survey. Data from these baseline P-SAFE assessments indicated patients’ aggregate mean out-of-pocket costs were $C401/28 days (median $C84, range $C0–$C4475), with an additional $C249/28 days related to imputed travel and parking (median $C80, range $C0–$C2680) (table 2). Patients reported lower mean monthly out-of-pocket costs and travel costs during subsequent P-SAFE surveys (at 6 and 12 months of follow-up); however, fewer patients completed these additional surveys (table 2). Death dates were available for 34 of the 56 patients who completed at least one P-SAFE survey. Of these 34, 33 completed a P-SAFE survey in their last year of life (table 2).
Patients’ monthly out-of-pocket costs and travel costs
The most frequently reported out-of-pocket costs were in the categories of prescription drugs, vitamins and supplements, and ‘other’ costs (primarily over-the-counter medications and travel costs). Costs related to in-home healthcare, other healthcare providers and family care were infrequently reported (ie, only 5/110 P-SAFE surveys reported costs in these categories). Costs related to complementary and alternative therapies, overnight stays and meals, and ‘other’ expenses made up the bulk of patients’ out-of-pocket costs (figure 1).

Patients’ mean monthly out-of-pocket costs by category. P-SAFE, Patient Self-Administered Financial Effects.
Perceived financial burden
17 of 56 participants (30%) perceived their financial burden to be high (ie, ‘somewhat’, ‘large’ or ‘worst possible’ financial difficulty, as per Longo et al3) as reported during their baseline P-SAFE (figure 2). This proportion dropped during subsequent P-SAFE surveys (19% at 6 months of follow-up and 11% at 12 months of follow-up); however, fewer patients completed these additional surveys.

Patient-perceived financial difficulty caused by cancer-related expenses.
Those reporting the lowest difficulty (‘no financial difficulty’) on their baseline P-SAFE reported mean monthly out-of-pocket costs of CA$88 (median $25), whereas those with “large financial difficulty” had mean out-of-pocket costs of $C1466 (median $C393). The participant reporting ‘worst possible financial difficulty’ did not report any out-of-pocket costs on their baseline P-SAFE.
Patients reporting high financial burden (ie, ‘somewhat’, ‘large’ and ‘worst possible’ financial difficulty) on their baseline P-SAFE were more likely to be younger and non-white (table 3). Gender, marital status, educational attainment, place of residence or income was not associated with patient-perceived financial burden.
Perceived financial burden (from baseline P-SAFE) by demographics
Asset decisions
As reported on their baseline P-SAFE survey, 34% of patients had to draw on their financial assets in order to pay for the costs of their care (figure 3). This included things such as withdrawing savings, borrowing money or downsizing their home. 66% of patients reported not having to make any such asset decisions.

Asset decisions made to cover cancer-related costs. *‘Other’ includes borrowing money from family/friends, using credit cards, using health spending account allowances.
Impacts of advanced cancer on employment
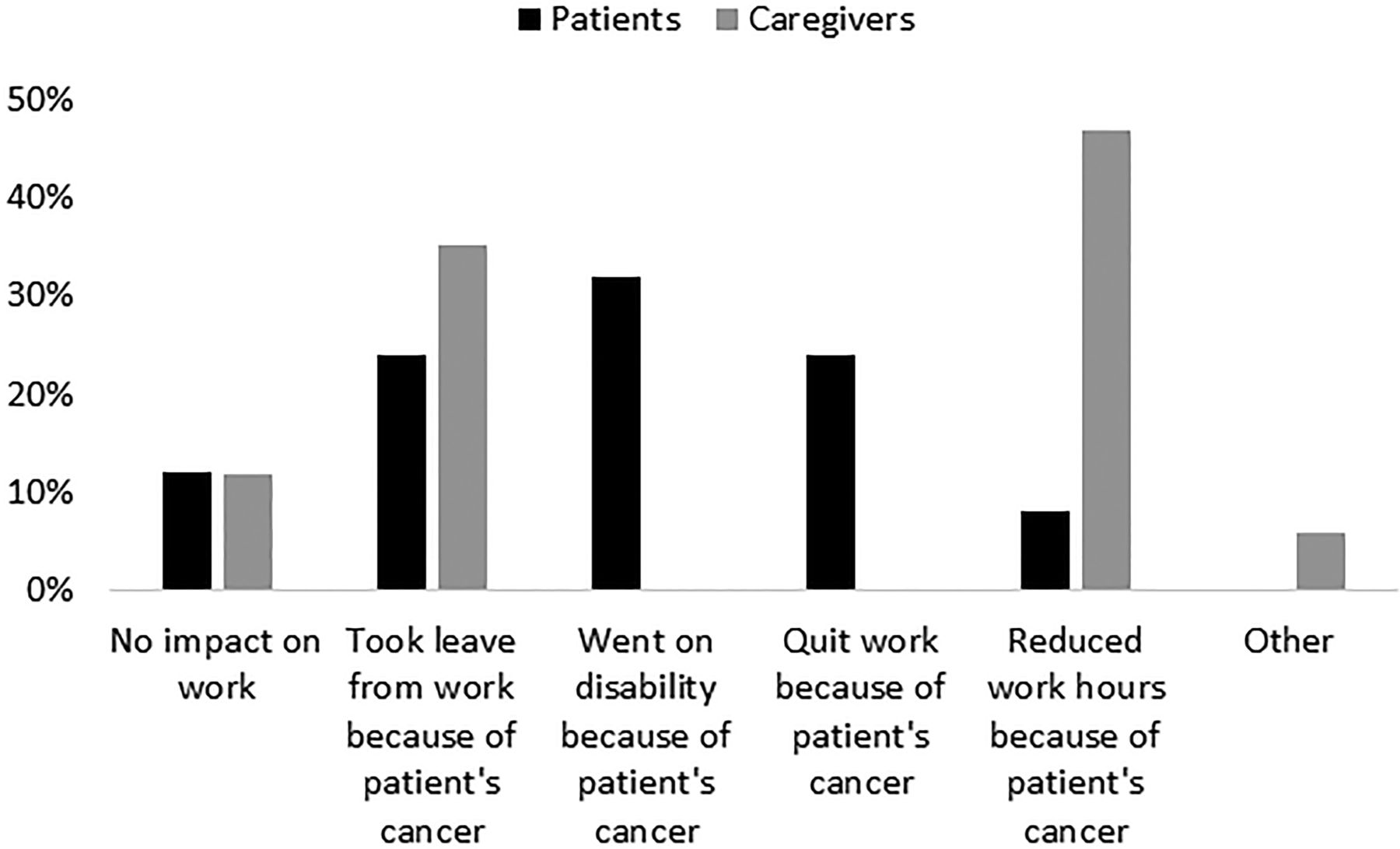
As reported on their baseline P-SAFE survey, 25 patients were deemed ‘eligible to work’; the other 31 patients reported being retired or unemployed by choice (eg, self-described ‘homemaker’) at the time of data collection and so were excluded from the analysis on impacts of cancer on employment. Patients were asked to identify up to three caregivers (ie, family or informal caregivers) who routinely provide care for them and to describe any impacts on their employment. Patients identified 40 caregivers, of whom 17 were eligible to work.
88% of work-eligible patients and 88% of work-eligible caregivers reported impacts on their employment (figure 4). Patients were most likely to take leave from their job and/or receive disability benefits, whereas caregivers were most likely to reduce their work hours.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Impacts of advanced cancer on patient and caregiver employment. Other: ‘medical issues so not working’.
Travel burden
Patients reported making several trips per month to their cancer centre, hospital, lab and/or pharmacy, with some patients travelling as far as 500 km one-way (5 hours) to their cancer centre (table 4).
Travel burden associated with advanced cancer
Discussion
This study sought to identify patient and family financial burdens (objective financial costs and subjective financial distress)12 specifically related to living with advanced colorectal cancer. Similar to a previous survey of Canadian patients with cancer,3 our study confirms that about one-third of patients perceive the financial burden of cancer to be ‘somewhat, large or worst possible’, despite living in a country with publicly funded healthcare and social benefits such as employment insurance. Data from patients’ ‘baseline’ P-SAFE assessments, which represented a cross-section of patients at varying time points from diagnosis of advanced cancer and at varying months of enrolment in the study, indicated their mean monthly out-of-pocket costs were $C401/28 days. A recent expanded analysis of the 2016–2019 survey of Canadian patients with cancer by Longo et al showed Albertan patients with cancer having the highest monthly out-of-pocket costs ($C938), travel costs and income loss. However, this analysis included patients with varying stages of disease and tumour types (breast, colorectal, lung and prostate).13
This study is notable for capturing longitudinal financial effects data from patients living with advanced colorectal cancer. This longitudinal analysis suggests that, not including lost employment earnings, although patients do show high out-of-pocket costs at baseline, these costs diminish over time with lower values 6 and 12 months later. This could be due to patients concluding active cancer treatment and requiring fewer medications/prescriptions and/or fewer trips to receive treatment. However, the data from patients’ last P-SAFE survey before death indicate that per patient out-of-pocket costs are also high in the last year of life, which is consistent with the Canadian cancer microsimulation model analysis, where the per patient costs (direct and indirect) are high during initial care (first 12 months after diagnosis), with a significant drop during ongoing care, followed by an increase again during the terminal phase of care (12 months before death).1 As in other studies,14–17 we found perceived financial burden was also associated with inequity, as those reporting higher burden were more likely to be non-white and younger.
Limitations
This sample was taken from two tertiary cancer centres and included rural-dwelling patients receiving treatment at the urban tertiary centres, who experienced higher travel/transportation costs than urban-dwelling patients. As such, the results are not generalisable to those treated only in community cancer centres.
Our sample may be subject to selection bias in that the included participants (64% of eligible patients in the larger ‘Living with Colorectal Cancer’ study) self-selected to provide recurrent financial effects survey data. It is possible their data may differ from the general colorectal cancer population, specifically, that this self-selection may have led to underrepresentation of certain groups (eg, those with the most severe financial burden or the least ability to participate). However, there were no statistical demographic differences between the P-SAFE and non-P-SAFE cohorts.
Our study sample is also somewhat heterogeneous in that patients were enrolled at various stages in their illness trajectory (ie, from date of diagnosis of advanced colorectal cancer), and they also completed P-SAFE surveys at varying months of enrolment in the study because of P-SAFE roll-out mid-way through the study.
Lastly, we did not assign a dollar value to patients’ and caregivers’ lost earnings from employment as respondents provided limited data in this section of the P-SAFE questionnaire, but nearly all employed or ‘work-eligible’ patients and their caregivers reported categorical impacts on their employment, which is consistent with previous reports in the literature.2 3 Our experience may help refine the P-SAFE questionnaire going forward.
Policy and practice implications
Patients’ out-of-pocket costs and financial burden are likely to increase from year to year with rising costs of living and high costs of novel cancer treatments.18 Several Canadian articles have provided recommendations for managing cancer-related financial toxicity,2 18–20 and a multipronged approach is likely to have the biggest impact. Healthcare providers are encouraged to have conversations with patients early and often, to help them address the potential financial impact and to refer them to available resources, for example, government or community financial assistance programmes, cancer centre financial navigator(s) if available and patient support groups.2 19 This would be especially important for those facing structural inequities like people living in rural and underserved areas. Using virtual visits or telephone follow-up assessments when possible, and arranging follow-ups with physicians closer to the patient’s home, may help reduce travel costs.2 21 Cancer centres are encouraged to implement routine screening for financial toxicity.2 Essue et al recently demonstrated the feasibility of a novel measure of health-related out-of-pocket cost burden experienced by households with a cancer patient/survivor, using routinely collected data, that could be leveraged to systematise the ongoing monitoring of financial burden in cancer populations.20
Policy changes to reduce cancer treatment costs and discourage the use of low-value cancer interventions can ease financial strain on patients.19 For example, expanding government-subsidised coverage for common prescription medications, high-cost medications and complementary treatments could significantly reduce out-of-pocket expenditures for advanced cancer patients. Cancer centres can seek to minimise travel through virtual appointments where appropriate and same-day treatments. Governments could explore expanding the care plans offered by pharmacists or nurse practitioners or family physicians to allow some routine checkups to be carried out in designated local pharmacies or community clinics. In their recent commentary, Wood and Murphy advocate for more comprehensive federal and provincial policies on costs for home care and medical equipment and expanding eligibility requirements for the Canada Pension Plan disability benefit.18
Conclusions
Despite having a publicly funded healthcare system, a significant proportion of people living with advanced cancer in Alberta, Canada experience high financial burden. A multipronged approach involving frontline providers (referring to available resources), cancer centres (adopting routine screening for financial distress, reviewing policies around virtual visits and same-day treatments) and governments (expanding drug plans, increasing disability and supportive leave benefits) is needed to mitigate cancer patients’ financial burden.
Data availability statement
Data are available on reasonable request. Aggregate, deidentified data may be made available on reasonable request from the corresponding author. The data are not publicly available, consistent with the ethics approval.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Health Research Ethics Board of Alberta Cancer Committee (HREBA-CC), study ID HREBA.CC-17-0429. Participants gave written, informed consent to participate in the study before taking part.
Acknowledgments
We thank all of the patients and staff at the cancer centres for their contributions to this study.
References
Footnotes
JS and AS are joint senior authors.
Presented at This work has been presented in part at the following conferences: 3rd and 4th Joint Sapporo Conference for Palliative and Supportive Care in Cancer, 27 April 2023–29 April 2023, Sapporo, Japan; 23rd International Congress on Palliative Care, 18 October 2022–21 October 2022, Montreal, Canada; MASCC/ISOO 2022 Annual Meeting, 23 June 2022–25 June 2022, Toronto, Canada; Canadian Cancer Research Conference (CCRC) 2021, 8 November 2021–11 November 2021 (virtual); 2021 Canadian Association for Health Services and Policy Research (CAHSPR) Annual Conference, 19 May 2021–21 May 2021 (virtual); 2021 Canadian Centre for Applied Research in Cancer Control (ARCC) Conference, 17 May 2021–18 May 2021 (virtual); 2021 Hospice Palliative Care Ontario (HPCO) Annual Conference, 18 April 2021–20 April 2021 (virtual); 11th World Research Congress of the European Association for Palliative Care (EAPC), 8 October 2020–9 October 2020 (virtual). This work has been published in part through the following conference abstracts: Supportive Care in Cancer 2022; 30(Suppl 1):S129, https://doi.org/10.1007/s00520-022-07099-y; Palliative Medicine 2020; 34(Suppl 1): 169, https://doi.org/10.1177/0269216320958098.
Contributors JS, AS, ME and SW conceived of the study. JS, AS, ME and SW acquired the funding. JS, AS, ME, PB and SW contributed to the study design including developing the study protocol, designing/selecting the data collection tools and developing the analysis plan. BME and CJL provided expert advice on collecting financial effects data and use of the P-SAFE tool. SK and CB were responsible for recruitment of study participants and collection of data. PB, ME, PS, PA and AS all participated in data analyses. All authors participated in data interpretation. PB drafted the manuscript and all authors have reviewed and critically revised it. All authors have read and approved the final manuscript. AS is responsible for the overall content of the manuscript and acts as guarantor.
Funding This work was supported by a Canadian Institutes of Health Research Operating Grant: Partnerships for Health System Improvement for Cancer Control (HRC-154127).
Competing interests AS has received an honorarium and travel expense reimbursement from the Canadian Society of Palliative Medicine and travel expense reimbursement from the Canadian Partnership Against Cancer. AS has an academic contract with Queen’s University, a leadership position with Lakeridge Health, an academic position with University of Calgary (non-financial) and a clinical position with Alberta Health Services.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.