Article Text

Abstract
Background In recent years, there has been an increased demand for non-pharmacological, complementary therapies and psychosocial provisions in hospices, aimed at creating spaces for communication and personalised expression in response to the bio-psycho-socio-existential needs of patients and their caregivers. As a contemporary evidence-based professional practice, music therapy is an integral part of multidisciplinary teams in many palliative care settings internationally. In Italy, however, music therapy is a developing area of practice facing certain challenges around professionalisation, funding and service development. This study seeks to explore the current state of music therapy in Italian hospices.
Methods From January 2024 to March 2024, an online survey was disseminated to 213 hospices across Italy. The survey consisted of 10 closed-ended questions. Data was analysed using descriptive statistics.
Results A 73.7% completion rate was achieved. Music-based interventions are provided in 49.6% of hospices (n=62), and 43.5% of these offer a music therapy service led by a qualified music therapist. Most hospices (n=17) offer music therapy sessions for 3 hours per week. Across all hospices, sessions are primarily individual and take place in patients' rooms. The presence of caregivers varies, and patients are referred to music therapy by different professionals in the team. Information was gathered regarding the use of music therapy during sedation and for bereavement support of caregivers, along with details on assessment tools used.
Conclusion This study offers an initial overview of music therapy in hospices across Italy and highlights critical questions regarding team integration, training standards, evaluation and funding.
- Hospice care
- Palliative Care
- Quality of life
- Supportive care
- Complementary therapy
- Bereavement
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Music therapy is an evidence-based professional practice supporting patients and caregivers in response to the bio-psycho-socio-existential needs in palliative care.
WHAT THIS STUDY ADDS
This study offers an initial overview of the provision of music therapy in Italian hospices and advances our understanding about current practice and service provision in palliative care.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Quality standards, training standards and multidisciplinary team integration emerge as key questions for music therapy provision in palliative care in Italy, and future studies on the impact and effects of music therapy in palliative care are encouraged.
Introduction
The World Health Organization (WHO) estimates that more than 56.8 million people worldwide need to receive palliative care each year. However, only 14% of these people receive palliative care.1 In Italy, the need for palliative care in the adult population is estimated to be between 1% and 1.4%. In the end of life, the incidence is about 293 000 patients per year, 60% of whom have chronic degenerative non-oncologic diseases and the remaining 40% have cancer.2
Palliative care aims to improve quality of life, alleviate suffering and manage physical, psychological, social and spiritual pain in individuals of all ages living with incurable diseases, particularly those in the end stages of life. Adopting a holistic approach, palliative care involves an interdisciplinary and multi-professional team approach supporting not only patients but also their caregivers during illness and in the bereavement process.
Music is an integral part of this holistic approach, and a range of musical care practices are observed in palliative care, including live music performance, community choirs and music thanatology practices. Such practices can be mapped across a ‘specialist-everyday’ and a ‘private-public’ continuum of care.3 As such, some musical care practices may involve, for example, a qualified music therapist facilitating an individual session with a patient retaining clear therapeutic boundaries and respecting the person’s privacy and confidentiality. Other musical care practices, however, may pertain to live music events within open community settings for death education purposes.4
Forming a distinct professional field of practice alongside other music-based interventions,5 music therapy has received increased attention in the past decades as an integrative non-pharmacological intervention in palliative care (figure 1). As a fundamentally relational practice,6 music therapy adapts according to each person’s needs and each setting, and it has diverse applications across a musical care continuum—including individual, group and community-oriented applications. The relevance and prioritisation of such applications are informed by numerous factors, including the music therapist’s training background and approach, as well as wider professional and sociocultural agendas.

Different types of music-based interventions in healthcare and medical settings. The figure is based on Stegemann et al.5 “Music therapy and other music-based interventions in paediatric healthcare: an overview”.
For the purposes of this study, the lead researchers (MB and FG) focus on the role of music therapy within a specialist domain of end-of-life care with particular reference to hospice care. Conceptualising music therapy in this context as ‘medical music therapy’ (MMT), they focus on music therapy as a specialist intervention led by a qualified music therapist and taking place within a private space dedicated to a person’s care. More particularly, they draw on Dileo’s concept of MMT7 and focus on the application of music therapy for the prevention, treatment and continuing care of persons who have medical conditions. Through this conceptualisation of MMT, their intention is to highlight the differences between music therapy and other music-based interventions in Italian medical care settings and to avoid potential misconceptions of music therapy often caused by the gaps in professional regulation across the country.8
MMT in palliative care can be used to support both the patient and their families, offering a holistic response to their expressed needs, alleviating pain,9 10 promoting communication and social outcomes11 and facilitating relationship completion at the end of life12 through individualised and personalised interventions. Furthermore, MMT seems to be more effective than other music-based interventions in palliative care,9 allowing the use of diverse methods and techniques and, therefore, promoting flexibility and reflexivity of music therapists. Although the provision of MMT in palliative care is developing in Italy, there is a lack of knowledge about its application, and there is no national picture of such provisions.
The aim of this study was to map the provision of MMT in Italian hospices. By exploring different aspects pertaining to the organisation and application of MMT, the study seeks to advance our understanding about current practice and service provision in palliative care.
Methods
Survey design
Based on a published survey focused on music therapy in paediatric oncology,13 the two lead researchers developed a survey using Google Form (online supplemental material 1).
Supplemental material
The opening of the survey offered information about the study and its ethical considerations. Following a consenting checkbox, the survey had two parts. The first part collected demographic information regarding the respondents and their hospice context (eg, hospice name, location and overall number of patient beds). The second part of the survey aimed to investigate how MMT is integrated into the care provided in each hospice setting. This part consisted of 10 questions following skip logic.
The first two questions were completed by all respondents and focused on whether a music-based intervention was being used at the hospice and by whom (ie, medical doctors, nurses, music therapist or others). The remaining eight questions were filled out only by respondents working in hospices where music-based interventions were provided by a qualified music therapist. These questions focused on MMT in relation to weekly duration of provision/contact time, session format (individual or group), participation of caregivers, location, referral, assessment, use of MMT during sedation and bereavement support (table 1).
Survey sections and questions
Respondents were invited to answer based on current practice and policies within their respective setting and not personal views.
Sampling
Italian hospices were screened from ‘Agenzia Nazionale per i Servizi Sanitari Regionali’ AGENAS14 by five music therapy master students (NB, AG, CM, MN and ES) from the ‘A. Vivaldi’ Conservatory of Alessandria. According to our inclusion criteria, the study was addressed to hospices which offer adult palliative care, were still open after 2022, have at least seven beds and employ a multidisciplinary team.
As such, some hospices, which were included in the AGENAS list, were not included in this survey as their small bed numbers did not justify the establishment of a multidisciplinary team and, therefore, the inclusion of MMT. Also, the study’s criteria regarding bed numbers were due to the Italian context where there is a difference between palliative care provided by the hospital and the territorial/community services provided at home and hospices that are residential. Although hospitals, territorial services and hospices are part of the same network, they have different teams. Accordingly, we did not include hospices, which were closed after the AGENAS survey, territorial-nonresidential palliative care units or other centres caring for people in a vegetative state.
Data collection and analysis
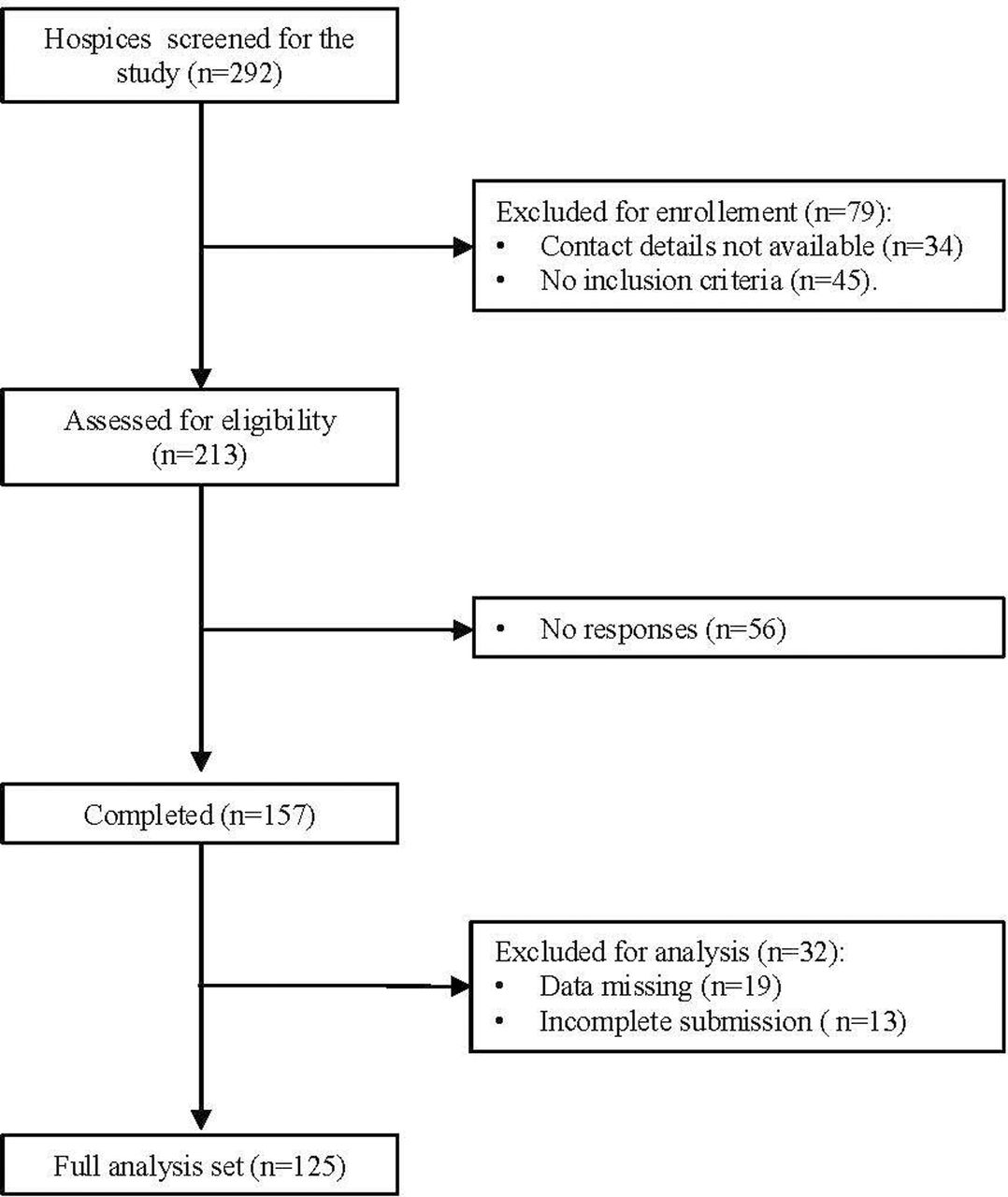
A total of 292 hospices were screened. 79 were excluded due to unavailability of contact details (n=34) and not meeting the inclusion criteria (n=45). In total, 213 hospices met the inclusion criteria. An email with the survey link was sent to the lead of each hospice’s multidisciplinary team, while information about the study was also disseminated through the newsletter of the Italian Society of Palliative Care.
Data was collected between January and March 2024, and 157 responses were received (one response per hospice). Overall, 56 hospices did not respond, and 32 were excluded from the analysis. An independent researcher (TM) downloaded all survey responses and analysed them using descriptive statistics. In total, 125 out of 157 responses were included in the dataset (figure 2).
As such, the completion rate was 73.7%, and the response rate was 58.7%.

Flow chart.
Results
Out of the 125 hospices included in the analysis, music-based interventions were provided in 62 hospices (49.6%).
Music therapy is provided in 27 of these hospices (43.5%) by a qualified music therapist. In most hospices (n=17; 63%), music therapy provision (contact time) is less than 3 hours per week. In nine hospices, weekly music therapy provision is between 3 and 10 hours, and only in one hospice is more than 10 hours per week (figure 3a).

{kind=link}
{kind=link}
{kind=link}
(a) Duration of weekly provision of music therapy per centre. (b) Format of music therapy sessions. (c) Presence of caregivers during the music therapy sessions. (d) Duration of weekly music therapy provision and session space. (e) Professionals making music therapy referrals. (f) Assessment tools. (g) Use of music therapy during sedation.
In terms of music therapy format, individual sessions are most common compared with group sessions [23 (85%) vs 4 (15%)] (figure 3b). Caregivers are commonly present in music therapy sessions (figure 3c).
In most hospices, music therapy sessions are offered in a dedicated room or in the patient’s room. The location of music therapy provision seems to depend partly on the number of hours that music therapy is provided in the setting each week. In hospices where music therapy is provided up to 3 hours/week, sessions are mainly delivered in a dedicated room (n=15) rather than the patient’s room (n=3) or other places (terrace (n=1)). Instead, when the music therapy provision increases (from 3 to 10 hours/week or over), the most used location is the patient’s room (figure 3d).
Referral pathways of patients to MTT vary. Frequently, the referral was made within multidisciplinary teams (35%) and less commonly by individual nursing staff (14%), medical staff (13%), the department lead (18%) or psychologist (3%) (figure 3e).
The assessment of MMT was mainly done through bespoke assessment tools developed by the music therapist (51%) or by other team members (31%). More rarely, music therapists used a validated assessment tool or scale (9%), and in four hospices (9%), no assessment was implemented (figure 3f).
The use of MMT during sedation did not feature much across hospices. In 44% of cases, music therapy was never used during sedation and rarely in 41% of cases (figure 3g).
Similarly, no use of MMT was reported in relation to grief support in most hospices (78%).
Discussion
This survey focused on 27 Italian hospice settings where music interventions were offered by qualified music therapists in line with professional standards of music therapy internationally.15 16 Interestingly, in 35 hospices, music-based interventions were offered by other professionals in the team (eg, medical staff, nursing staff, psychologist, occupational therapist or art therapist), professional musicians, family members or volunteers. These settings were excluded from our analysis, but future research could explore such practices and explore possibilities for cross-professional collaboration and exchange while retaining clear professional roles and boundaries.
The number of hospices employing a music therapist is low (n=27; 12.6%) compared with the overall number of hospices contacted and even lower (9.2%) when compared with the 292 hospices and palliative care centres surveyed by AGENAS in 2021. It becomes clear that most hospices in Italy do not employ a music therapist and have no music therapy provision. Despite the lack of international data, a recent mapping of arts services in hospices across Scotland shows that music therapy is available in almost one-third of the hospices nationally.17 Earlier studies also indicated palliative and end-of-life care as a growing area of practice for music therapists in the UK18 and in the USA.19 In many countries within the Mediterranean region,20 however, the field of music therapy faces certain challenges often related to funding and professionalisation issues, including the lack of regulation. Such issues seem to be connected to misperceptions around professional identities, and they can be a barrier to the smooth integration of music therapy services within each country’s healthcare system.
This survey’s framing of music therapy as MMT relates to such challenges aiming to highlight music therapists’ qualification and specialisation as healthcare professionals who practice as members of the multiprofessional team within medical and other healthcare settings. Differently to other music-based interventions,21 22 MMT as an evidence-based practice works towards specific aims in palliative care to meet the patient and the family needs and interests as an integral part of the interdisciplinary team. Music therapists work with flexibility to meet the person, and their practice in hospices can be understood on a supportive, communicative/expressive and transformative level.11
MMT practice in Italian hospices seems to focus on the specialist-private domain, as outlined earlier. However, examples from other countries highlight the diversity of music therapy work and approaches. Music therapists, for example, provide environmental music therapy to influence organisational well-being. They may coordinate live music events for health promotion and community engagement, and they may facilitate community choirs and lead music-based death education intergenerational projects.23
Most Italian hospices provide MMT up to 3 hours per week. This limited provision poses challenges and barriers to effective multidisciplinary communication and integration.24 These challenges are particularly evident given the potentially rapid changes in patients’ health conditions whose hospice stay varies in length. The ability to respond to people’s changing needs and work with flexibility is key in palliative care. Equally, best music therapy practice in hospices calls for the ability to adjust and increase, if and when needed, the frequency and duration of sessions depending on fluctuating patient referrals and people’s changing conditions, which must be assessed on a case-by-case basis.
The limited number of music therapy hours provided in most hospices across Italy indicates potential education, funding and policy issues in the field. Despite the existence of a public academic training programme (Master’s degree and PhD in Music Therapy) established by the Italian Ministry of University and Research in line with international training standards, the provision of music therapy services is weakly supported by the State and is primarily funded by foundations and/or private associations. Further, the Italian law for new professions seems insufficient for offering a national professional framework for music therapists working in hospice or other medical settings where there might be a need for advanced skills and specialised training with a focus on interdisciplinary collaboration. This is in line with Cheryl Dileo, who points out the necessity of skills and advanced and specialised training to work in this context, in particular a high level of interdisciplinary skills. This situation limits the sustainability and expansion of music therapy services in Italy, and future cross-national studies can help compare the MMT practices in hospices in other countries, analysing cultural, organisational and professional differences.
In our survey, individual MMT sessions were conducted in 23 hospices. Such provision is key to the personalised care,25 as a fundamental palliative care principle, and can be an important part of Advance Care Planning.26 The necessity to design personalised individual interventions requires a person-centred approach to MMT,27 which takes into consideration the needs of the patient and/or caregivers.27–30
In four hospices, MTT was provided in group sessions, involving more than one patient and potentially family members. Although the provision of group sessions is common in other music therapy settings (eg, schools, care homes and community centres), groups tend to be less common in hospice care. Examples from international literature highlight the application of group work in relation to death education programmes and health-promoting palliative care initiatives.23 Future research could explore further the relevance and scope of group MMT in Italian hospice settings.
The use of a dedicated music therapy room seems important for hospices that focus on MMT within a specialist-private domain. In line with the survey findings, however, increased hours of weekly MMT provision seem to relate to an expanded use of spaces beyond a dedicated room to include the provision of sessions in patients’ rooms. This expansion may indicate an increased multidisciplinary team integration that allows for more shared understanding of what is being offered, where and how. The increased fluidity of spaces used for MMT may enable a greater ability to meet the person’s needs and optimise the music therapist’s work. However, such fluidity needs to be navigated carefully while considering its potential negative impact in terms of creating a safe uninterrupted therapeutic space. Future research could explore to what extent the choice of session location is led by clinical reasons (eg, limited mobility of patient) and/or practical reasons (eg, unavailability of other spaces).
The survey findings call for a critical reflection around the criteria for referrals to MMT as these are carried out by different people. The need to share clear criteria and pathways for referral to MMT in relation to the specific modalities, timing, goals and patient needs is highlighted. Building on existing knowledge regarding how hospice services are organised in Italy, future research can focus on the referral criteria for patients (and potentially caregivers) to MMT, unpacking different potential perspectives and motivations among professionals to include clinical, psychological, spiritual or other aspects. Additionally, it is important to explore further how the referral process unfolds through the multidisciplinary team.
Music therapy assessment is essential and should relate to the multidimensional assessment of needs that the patient and/or their caregivers present. In fact, the assessment of care needs and priorities is fundamental to hospice outcome measurement and is implemented according to timelines defined by the multidisciplinary team with instruments such as the Integrated Palliative Care Outcome Scale (IPOS).31–33 The survey findings show that music therapists in Italian hospices mainly use bespoke evaluation instruments that they have personally developed (51%). Two hospices specified that an observation form and a questionnaire were used to collect information about aspects and outcomes related to emotional and verbal expression, interpersonal relationship, sound-music/listening dynamics and session enjoyment. In other cases, music therapy assessment was done based on tools created by different team members (31%) or validated assessment scales/tests (9%). A combined use of such tools can provide a more comprehensive assessment of the patient’s care process in music therapy. Further studies are needed to explore music therapy assessment practices within hospices while considering trends and challenges in outcome measurement in the wider music therapy field.34
The study found that MMT in palliative sedation is rarely used in 41% of hospices where music therapy is available. Therapeutic palliative sedation is the relief of refractory suffering through the monitored proportional use of medications intended to reduce consciousness in patients with life-limiting diseases.35 In some cases, sedation still allows for some interaction with the patient, and it is possible to propose receptive music therapy particularly for patients who have already had music therapy sessions, have established a safe therapeutic relationship and whose preferences are known. The literature lacks studies on the use of music therapy with patients in deep sedation.36 The hypothesis is that in this case, receptive music therapy can be proposed as an additional supportive resource alongside other resources such as therapeutic touch.37 Furthermore, future studies are recommended to deepen the understanding of the impact that music therapy might have on family members in relation to anticipatory grief and bereavement38 39 within or beyond the hospice context.
Conclusions
The conception of MMT, underpinned by a professional agenda for the promotion of the music therapy profession in healthcare contexts in Italy, highlights the specialised qualification of music therapists and how they work with therapeutic intent and clinical reasoning. This conception challenges assumptions of perceived overlaps between music therapy and other music-based interventions offered by non-music therapists in hospices. This is crucial in Italy and other countries where the lack of professional registration poses barriers and risks to professional integration, safe practice and service development. While we recognise a need to move beyond a traditional medicalised model of palliative care, we highlight the need for clear education, professional and policy frameworks for music therapy practice. The survey findings stimulate reflection on quality standards, and future directions may include establishing a network of music therapists working in Italian hospices to work towards shared criteria and best practices. Additionally, future studies on the impact and effects of MMT in hospice care in Italy are encouraged.
Limitations
The findings of this study should be interpreted considering its limitations.
Despite the good response rate, the data collected in this study does not fully represent the reality of Italian hospices. The survey data represent local hospice services and not individual opinions. Although this approach may reduce subjectivity, it could lead to standardised responses that do not fully reflect the variability in daily practice. The study also did not focus on the impact of MMT in the clinical and organisational setting, but future research may explore this.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
No ethics approval was required. Data was collected and stored in line with the General Data Protection Regulation (GDPR) principles and the Helsinki Declaration.
References
Footnotes
Contributors MB and FG formulated the research design and drafted the paper. AM collaborated on formulating the research idea and provided critical review of the manuscript. TM collated the dataset and completed the statistical data analysis. NB, AG, CM, MN and ES helped with data collection and critical review of the manuscript. GT provided critical review of the manuscript and contributed to re-drafting sections of the paper. FG is is the guarantor under author contributions statement.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.